Efficacy
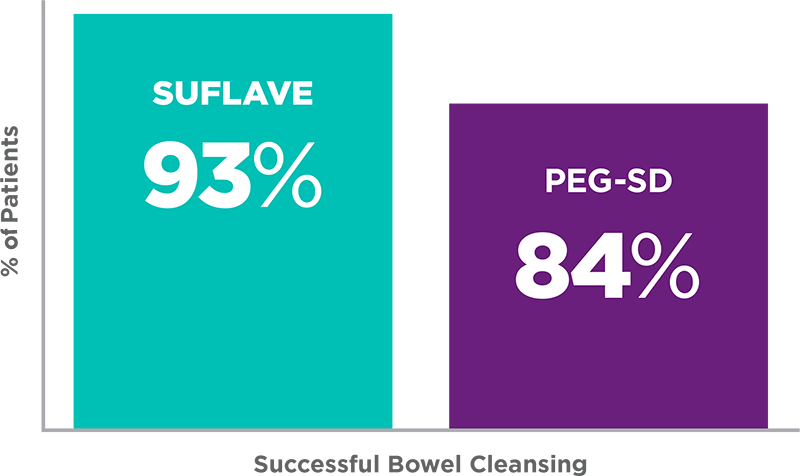


SUFLAVE® provided higher efficacy rates compared with PEG-SD: 93% vs 84%, respectively5†
- Blinded central readers rated SUFLAVE® efficacy higher than PEG-SD; P<0.055:
- 98% vs 74% of SUFLAVE® vs PEG-SD patients reported a better overall preparation experience (ratings of excellent to good)
Study Design3,5: This multicenter, non-randomized, unblinded, phase 2 trial assessed 60 subjects. Since performing endoscopists were unblinded, blinded central reading was also performed using colonoscopy videos. Subjects assigned to PEG-SD received two 5-mg OTC bisacodyl laxative tablets, two 32-ounce bottles of lemon-lime–flavored sports drink (Gatorade®), and two 119-g bottles of polyethylene glycol 3350 (PEG 3350). The primary endpoint was the percentage of subjects with successful cleansing, which was based on the US FDA Bowel Prep Scoring Scale. The goal of the study was to evaluate SUFLAVE® vs PEG-SD.
*Success was defined as an overall cleansing assessment of excellent or good by the blinded endoscopist; scores were assigned following completion of the colonoscopy.
†Numerical differences based on local endoscopists’ ratings. Statistical comparisons were not performed due to unblinded endoscopists.
SD=sports drink.
Gatorade® is a registered trademark of Stokely-Van Camp, Inc.
SUFLAVE® (polyethylene glycol 3350, sodium sulfate, potassium chloride, magnesium sulfate, and sodium chloride for oral solution)
ADDITIONAL IMPORTANT SAFETY INFORMATION
Contraindications
SUFLAVE is contraindicated in the following conditions:
- Gastrointestinal obstruction or ileus [see Warnings and Precautions (5.6)]
- Bowel perforation [see Warnings and Precautions (5.6)]
- Toxic colitis or toxic megacolon
- Gastric retention
- Hypersensitivity to any ingredient in SUFLAVE [see Warnings and Precautions (5.8)]
Warnings and Precautions
-
Serious Fluid and Electrolyte Abnormalities: Advise all patients to hydrate adequately before, during, and after the use of SUFLAVE. If a patient develops significant vomiting or signs of dehydration after taking SUFLAVE, consider performing post-colonoscopy lab tests (electrolytes, creatinine, and BUN).Bowel preparation products can cause fluid and electrolyte disturbances, which can lead to serious adverse reactions including cardiac arrhythmias, seizures, and renal impairment [see Adverse Reactions (6.2)]. Correct fluid and electrolyte abnormalities before treatment with SUFLAVE. Use SUFLAVE with caution in patients with conditions, or who are using medications [such as diuretics, angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs)], that increase the risk for fluid and electrolyte disturbances or may increase the risk of seizure, arrhythmias, and renal impairment [see Drug Interactions (7.1)].
- Cardiac Arrhythmias: There have been rare reports of serious arrhythmias associated with the use of ionic osmotic laxative products for bowel preparation. These occur predominantly in patients with underlying cardiac risk factors and electrolyte disturbances. Use caution when prescribing SUFLAVE for patients at increased risk of arrhythmias (e.g., patients with a history of prolonged QT interval, uncontrolled arrhythmias, recent myocardial infarction, unstable angina, congestive heart failure, or cardiomyopathy). Consider pre-dose and post-colonoscopy ECGs in patients at increased risk of serious cardiac arrhythmias.
-
Seizures: There have been reports of generalized tonic-clonic seizures and/or loss of consciousness associated with use of bowel preparation products in patients with no prior history of seizures. The seizure cases were associated with electrolyte abnormalities (e.g., hyponatremia, hypokalemia, hypocalcemia, and hypomagnesemia) and low serum osmolality. The neurologic abnormalities resolved with correction of fluid and electrolyte abnormalities.Use caution when prescribing SUFLAVE for patients with a history of seizures and in patients at increased risk of seizure, such as patients taking medications that lower the seizure threshold (e.g., tricyclic antidepressants), patients withdrawing from alcohol or benzodiazepines, or patients with known or suspected hyponatremia [see Drug Interactions (7.1)].
- Use in Patients with Risk of Renal Injury: Use SUFLAVE with caution in patients with impaired renal function or patients taking concomitant medications that may affect renal function (such as diuretics, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, or non-steroidal anti-inflammatory drugs) [see Drug Interactions (7.1)]. These patients may be at risk for renal injury. Advise these patients of the importance of adequate hydration with SUFLAVE and consider performing baseline and post-colonoscopy laboratory tests (electrolytes, creatinine, and BUN) in these patients [see Use in Specific Populations (8.6)].
- Colonic Mucosal Ulcerations and Ischemic Colitis: Osmotic laxative products may produce colonic mucosal aphthous ulcerations, and there have been reports of more serious cases of ischemic colitis requiring hospitalization. Concurrent use of stimulant laxatives and SUFLAVE may increase these risks [see Drug Interactions (7.3)]. Consider the potential for mucosal ulcerations resulting from the bowel preparation when interpreting colonoscopy findings in patients with known or suspect inflammatory bowel disease.
-
Use in Patients with Significant Gastrointestinal Disease: If gastrointestinal obstruction or perforation is suspected, perform appropriate diagnostic studies to rule out these conditions before administering SUFLAVE [see Contraindications (4)].Use with caution in patients with severe active ulcerative colitis.
-
Aspiration: Patients with impaired gag reflex or other swallowing abnormalities are at risk for regurgitation or aspiration of SUFLAVE. Observe these patients during administration of SUFLAVE.Do not combine SUFLAVE with starch-based thickeners [see Dosage and Administration (2.1)]. Polyethylene glycol (PEG), a component of SUFLAVE, when mixed with starch-thickened liquids reduces the viscosity of the starch-thickened liquid. When a PEG-based product used for another indication was mixed in starch-based pre-thickened liquids used in patients with dysphagia, thinning of the liquid occurred and cases of choking and potential aspiration were reported.
- Hypersensitivity Reactions: SUFLAVE contains polyethylene glycol (PEG) and other ingredients that may cause serious hypersensitivity reactions including anaphylaxis, angioedema, rash, urticaria, and pruritus [see Adverse Reactions (6.2)]. Inform patients of the signs and symptoms of anaphylaxis, and instruct them to seek immediate medical care should signs and symptoms occur.
Adverse Reactions
Most common adverse reactions (≥2%) are: nausea, abdominal distension, vomiting, abdominal pain and headache.
These are not all the possible side effects of SUFLAVE. Please see Adverse Reactions (6) in the Prescribing Information for a full list.
Drug Interactions
Drugs that increase risk of fluid and electrolyte imbalance. (7.1)
To Report SUSPECTED ADVERSE REACTIONS, contact Azurity Pharmaceuticals, Inc. at 1-800-461-7449, or FDA at 1-800-FDA-1088 or www.fda.gov/MedWatch.
SUFLAVE® is a registered trademark of Azurity Pharmaceuticals, Inc.
PP-SUF-6488-US-EN-v1
View the Full Prescribing Information and Medication Guide.
References
1. SUFLAVE® [package insert]. Woburn, MA: Azurity Pharmaceuticals, Inc.
2. Bhandari R, Goldstein M, Mishkin DS, et al. Comparison of a novel,
SUTAB® (sodium sulfate, magnesium sulfate, and potassium chloride) tablets, for oral use
Indications and Usage
SUTAB is indicated for the cleansing of the colon as a preparation for colonoscopy in adults.
ADDITIONAL IMPORTANT SAFETY INFORMATION
Contraindications
SUTAB is contraindicated in the following conditions:
- Gastrointestinal obstruction or ileus [see Warnings and Precautions (5.6)]
- Bowel perforation [see Warnings and Precautions (5.6)]
- Toxic colitis or toxic megacolon
- Gastric retention
- Hypersensitivity to any ingredient in SUTAB [see Warnings and Precautions (5.7) and Description (11)]
Warnings and Precautions
- Serious Fluid and Electrolyte Abnormalities: Advise all patients to hydrate adequately before, during, and after the use of SUTAB. If a patient develops significant vomiting or signs of dehydration after taking SUTAB, consider performing post-colonoscopy lab tests (electrolytes, creatinine, and BUN). Fluid and electrolyte disturbances can lead to serious adverse events including cardiac arrhythmias, seizures and renal impairment. Correct fluid and electrolyte abnormalities before treatment with SUTAB. Use SUTAB with caution in patients with conditions, or who are using medications, that increase the risk for fluid and electrolyte disturbances or may increase the risk of adverse events of seizure, arrhythmias, and renal impairment [see Drug Interactions (7.1)].
- Cardiac Arrhythmias: There have been rare reports of serious arrhythmias associated with the use of ionic osmotic laxative products for bowel preparation. Use caution when prescribing SUTAB for patients at increased risk of arrhythmias (e.g., patients with a history of prolonged QT, uncontrolled arrhythmias, recent myocardial infarction, unstable angina, congestive heart failure, or cardiomyopathy). Consider pre-dose and post-colonoscopy ECGs in patients at increased risk of serious cardiac arrhythmias.
-
Seizures: There have been reports of generalized tonic-clonic seizures and/or loss of consciousness associated with use of bowel preparation products in patients with no prior history of seizures. The seizure cases were associated with electrolyte abnormalities (e.g., hyponatremia, hypokalemia, hypocalcemia, and hypomagnesemia) and low serum osmolality. The neurologic abnormalities resolved with correction of fluid and electrolyte abnormalities.Use caution when prescribing SUTAB for patients with a history of seizures and in patients at increased risk of seizure, such as patients taking medications that lower the seizure threshold (e.g., tricyclic antidepressants), patients withdrawing from alcohol or benzodiazepines, or patients with known or suspected hyponatremia [see Drug Interactions (7.1)].
- Use in Patients with Risk of Renal Injury: Use SUTAB with caution in patients with impaired renal function or patients taking concomitant medications that may affect renal function (such as diuretics, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, or non-steroidal anti-inflammatory drugs) [see Drug Interactions (7.1)]. These patients may be at risk for renal injury. Advise these patients of the importance of adequate hydration with SUTAB and consider performing baseline and post-colonoscopy laboratory tests (electrolytes, creatinine, and BUN) in these patients [see Use in Specific Populations (8.6)].
- Colonic Mucosal Ulcerations and Ischemic Colitis: Osmotic laxative products may produce colonic mucosal aphthous ulcerations, and there have been reports of more serious cases of ischemic colitis requiring hospitalization. Concurrent use of stimulant laxatives and SUTAB may increase these risks [see Drug Interactions (7.3)]. Consider the potential for mucosal ulcerations resulting from the bowel preparation when interpreting colonoscopy findings in patients with known or suspect inflammatory bowel disease (IBD).
-
Use in Patients with Significant Gastrointestinal Disease: If gastrointestinal obstruction or perforation is suspected, perform appropriate diagnostic studies to rule out these conditions before administering SUTAB [see Contraindications (4)].Use with caution in patients with severe active ulcerative colitis.
- Hypersensitivity Reactions: Serious hypersensitivity reactions, including anaphylaxis, angioedema, dyspnea, rash, pruritus and urticaria have been reported with SUTAB [see Adverse Reactions (6.2)]. Inform patients of the signs and symptoms of anaphylaxis and instruct them to seek immediate medical care should signs and symptoms occur.
- Risk of Gastrointestinal Complications with Ingestion of Desiccant: Each SUTAB bottle contains a desiccant. Remove and discard the desiccant from both bottles of SUTAB the evening prior to the colonoscopy [see Dosage and Administration (2.2)]. Postmarketing reports of patients ingesting the desiccant along with the SUTAB tablets has been reported and may be associated with risk of gastrointestinal complications and/or choking.
Adverse Reactions
Most common gastrointestinal adverse reactions are nausea, abdominal distension, vomiting, and upper abdominal pain.
These are not all the possible side effects of SUTAB. Please see Adverse Reactions (6) in the Prescribing Information for a full list.
Drug Interactions
Drugs that increase risk of fluid and electrolyte imbalance. (7.1)
To Report SUSPECTED ADVERSE REACTIONS, contact Azurity Pharmaceuticals, Inc. at 1-800-461-7449, or FDA at 1-800-FDA-1088 or www.fda.gov/MedWatch.
SUTAB® is a registered trademark of Azurity Pharmaceuticals, Inc.
PP-STB-6510-US-EN-v1
